
What makes hemophilia B unique.
Like hemophilia A, hemophilia B is a rare bleeding disorder that reduces the blood’s ability to clot, but there are important differences between the two.
Understanding what makes hemophilia B unique can help you work with your care team to develop a treatment and management plan that’s right for you.
All about factor IX
Both hemophilia A and hemophilia B are caused by a missing or deficient clotting factor. In hemophilia A, that’s factor VIII. In hemophilia B, it’s factor IX. It’s important for people with hemophilia B to know that factor IX has distinct characteristics and behaviors that can impact treatment and how it acts in the body.
The differences between factor IX and factor VIII
Factor IX moves through the body differently than factor VIII, creating a unique pharmacokinetic, or PK, profile.

Half-life
This is the amount of time it takes for factor level to go down by 50% after an infusion. The half-life of factor IX tends to be longer than the half-life of factor VIII.

Volume of distribution
This is a measure of how much factor is in the blood and in other tissues in the body. Volume of distribution tends to be higher in factor IX than factor VIII.

Clearance
This is the speed at which factor is eliminated from the body. Factor IX clearance is higher than factor VIII clearance.

Trough
This is the lowest level of factor activity right before an infusion. For people with hemophilia B, trough may not account for all the factor IX activity in the body.
Looking beyond trough levels
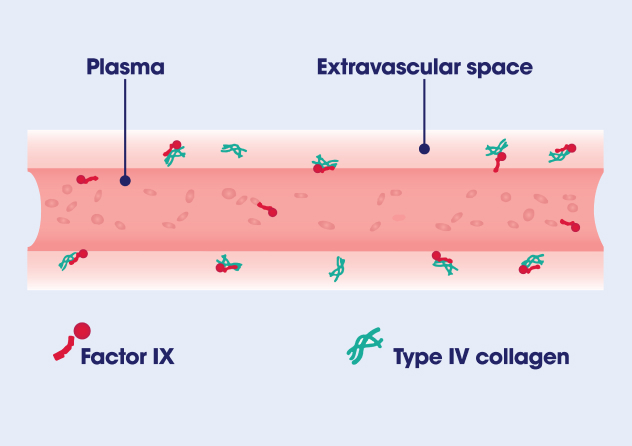
Unlike factor VIII, which only circulates in the bloodstream, factor IX is able to move outside of the bloodstream, in what’s called the extravascular space. Here, it binds to type IV collagen and allows factor IX to participate in the coagulation cascade to form clots and stop bleeds. This distribution into the extravascular space may be what gives factor IX a longer half-life.
Take a deeper dive into how clotting factors move in the body and how that can impact your treatment on our Pharmacokinetics and Factor Activity page.
LEARN MORETreating and managing hemophilia B
For people with hemophilia A, trough levels are often used to indicate when factor activity levels are at their lowest and help inform how often to infuse. However, because factor IX can exist in the extravascular space outside of the plasma, trough levels do not always reveal how much factor is in the body for people with hemophilia B. That’s why a more comprehensive PK assessment is often recommended.
The need for expanded PK profiles
Because trough levels are often not a reliable measure of how much Factor IX is in the body, it’s important to look at other pharmacokinetic parameters, too. A complete pharmacokinetic profile should assess at least six parameters, including half-life, trough, clearance, and volume of distribution. Assessing peak, or the factor activity levels right after an infusion, and the area under the curve (AUC), which is the amount of factor in the body over time, are also recommended. These parameters together can help determine how much factor therapy is needed, and how often.

Considering the whole person
Hemophilia treatment goes beyond analyzing factor activity levels. It’s about helping you take control of your health so you can live the life you want. Talk through these considerations with your care team to help shape a treatment plan that will work best for you.
Bleed rates
How often do you experience bleeds? Your bleed rate impacts what kind of therapy, and what administration schedule, is best for you.
Joint health
How are your joints? Bleeding in your joints can cause arthritis and other complications. Your need for joint bleed prevention is a key factor in determining treatment.
Lifestyle
What does your life look like? Your treatment plan should be designed to allow you to keep doing as many of your favorite things as possible.
More hemophilia B resources
Get the knowledge you need to redefine life with hemophilia B.



Discover a treatment option
Learn about an extended half-life treatment option for hemophilia B.

Joint Health
Take a deep dive into joint health and learn ways to recognize and manage bleeds.